ADVANCED ABDOMINAL/PELVIC EMERGENCIES |
IntroductionAbdominal and pelvic injuries in the pre-hospital environment pose a significant problem for the caregiver. Injuries to the abdomen and pelvis are not treated in an ambulance no matter what level of certification/license you are. These injuries are not treated in the Emergency Department in most cases. These wounds usually require operative intervention. Surgery is the only definitive care for most of these injuries. By understanding these injuries and their complications, you can be better prepared to handle the victim's needs and reduce mortality as well. AnatomyAbdominal CavityThe abdominal cavity is that portion of the torso commonly referred to as the "belly." Anatomically, the abdomen is bordered superiorly by the diaphragm which is the main muscle of the respiratory system. It contracts and "flattens" during inspiration and then relaxes, allowing for a gentle elevation, during exhalation. The diaphragm may rise to the level of the fifth intercostal space during exhalation, therefore, injuries to the thoracic region may result in injury to abdominal organs. The abdomen is bordered circumferentially by the peritoneal lining. Inferiorly, there is no true separation of the abdomen from the pelvic cavity other than its proximity. Posteriorly, the peritoneal lining separates the abdominal cavity from the retroperitoneal space. The abdominal cavity contains many solid as well as hollow organs: · The liver is the largest solid organ in the abdomen. It is a highly vascular organ that secretes bile, produces blood proteins, detoxifies drugs and other harmful substances, and converts glucose into glycogen for storage. The liver is partially protected by the right costal margin. · The gallbladder is a hollow organ that stores bile and releases bile into the small intestine for aid in digestion. · The pancreas is a solid organ that secretes digestive enzymes and is also an endocrine gland that produces the hormones insulin and glucagon. · The stomach is a large hollow organ that is a major organ of digestion. It is a muscular organ that functions in grinding food products into smaller components and also secretes powerful digestive juices. · The spleen is a highly vascular solid organ that filters blood for bacteria and other foreign particles. It is protected by the left costal margin. · The small intestine is a long hollow tube that is highly coiled so it will fit in the abdominal cavity. It functions in digestion and absorption of nutrients. The small intestine is divided into three sections: the duodenum, the jejunum, and the ileum. · The large intestine is a hollow organ composed of the colon and the rectum. The colon is divided into ascending, transverse, descending, and sigmoid regions. The large intestine contains bacteria which aid in digestion. The main function of the large intestine is reabsorption of water. · The appendix is a small hollow pouch that projects from the inferior portion of the ascending colon. It has no known function but is susceptible to inflammation and possible rupture. Retroperitoneal SpaceThe retroperitoneal space is located behind the abdominal cavity and contains the kidneys, the ureters, the aorta, and the inferior vena cava. The kidneys are two solid organs that are partially protected by the rib cage. They function in filtering blood and maintaining water balance in the body. Injuries to the kidneys may cause hematuria (blood in the urine). The ureters transport urine from the kidneys to the urinary bladder. Pelvic CavityThe pelvic cavity contains many structures as well. The pelvic cavity is protected by the pelvis, which is divided into the ilium, ischium, and pubis. The pelvic cavity contains the structures of reproduction and urinary excretion. · The urinary bladder is a hollow organ that stores urine and drains via the urethra. · The ovaries are the female reproductive organs that produce eggs (ova) and secrete different hormones during the monthly cycle and during pregnancy. · The fallopian tubes carry the egg to the uterus. · The uterus is a hollow muscular organ that is the location of fetal development during pregnancy. The uterus is connected by the cervix to the vaginal orifice. · The testes are the male organs of reproduction. They are located in the testicular sac and produce sperm and secrete male hormones. The sperm are discharged via the vas deferens into the penile meatus. Abdominal Quadrants
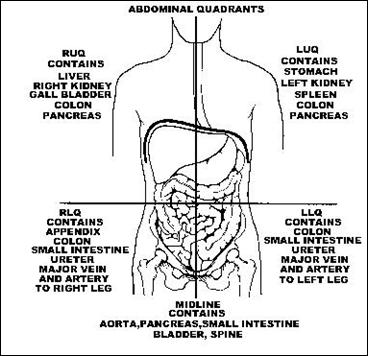
The abdomen is divided by two imaginary perpendicular lines that cross at the umbilicus. This divides the abdomen into four quadrants. · Right upper quadrant (RUQ) - liver, gallbladder, transverse and ascending colon, small intestine · Left upper quadrant (LUQ) - stomach, spleen, transverse and descending colon, small intestine · Right lower quadrant (RLQ) - appendix, ascending colon, small intestine
·
Abdominal and Pelvic InjuriesInjuries to the abdomen and pelvis occur as a result of blunt and penetrating trauma. This may be caused by deceleration forces such as those created by MVA's, explosions, knife, and gunshot wounds. The injuries most commonly seen in trauma to the abdomen include rupture of solid organs, lacerations of hollow organs, and eviscerations of abdominal contents. RuptureRupture of a solid organ leads to significant hemorrhage from that organ. Organs such as the liver and spleen are extremely vascular and therefore bleed considerably. Signs and symptoms of intra-abdominal bleeding include the following: · mechanism of injury consistent with injury · abdominal pain · distended abdomen · abdomen firm and painful upon palpation · tachycardia · developing shock Laceration Laceration of hollow organs within the abdomen may also bleed. They also lead to peritonitis or massive inflammation or the peritoneal lining. This inflammation may be caused by blood, digestive juices, and also by bacteria which are normally in the intestines to aid in digestion. When these microorganisms are allowed to spill into the peritoneal cavity, then peritonitis may occur. It is also important to note that liquids do not compress. Any hollow organ filled with a liquid medium is subject to compression secondary to trauma. This could lead to rupture of that organ. A good example is the urinary bladder. When full, such as after drinking a lot of beer, it may be compressed by the lap portion of the safety belt during an MVA. Rupture and significant hemorrhage could ensue. Signs and symptoms of lacerations to hollow abdominal organs may present late. Therefore, a high index of suspicion and continuous reassessments are imperative. Signs and symptoms include the following: · mechanism of injury · abdominal pain · rebound pain (pain when you quickly remove your hand during palpation) · developing shock Eviscerations Gunshot wounds and ripping lacerations of the abdomen may lead to abdominal eviscerations. This occurs when the skin and muscles covering the abdomen and the peritoneal lining are lacerated. This allows abdominal structures such as the small and large intestines to spill out of the body. This type of wound may cause the caregiver to have "tunnel vision." It is imperative that the rescuer perform an organized patient assessment so that other immediate life threats are not missed. Treatment of this wound requires the rescuer to cover the abdominal contents with a sterile bulky dressing moistened with normal saline. This should then be covered with plastic film wrap or aluminum foil. These are necessary to prevent the dressing from adhering to the intestines and to preserve heat loss respectively. The care giver should never attempt to reintroduce the intestines. This could lead to intestinal laceration, obstruction, or infection. Repair of an abdominal evisceration is a surgical procedure performed only by a physician. Injuries to the GenitaliaInjuries to the female genitalia usually result from direct trauma to the area. Forceful placement of objects in the vaginal canal can cause trauma and resulting external and internal bleeding. Child molestation and sexual assault are common sources of injury to this area. Injuries to the male genitalia are more common. These structures are highly vascular and have many nerve endings so injuries to this area are usually quite painful. Lacerations may result in severe bleeding and blunt trauma may result in a significant hematoma. Pelvic InjuriesInjuries to the pelvic cavity may be potentially life-threatening. Fractures of the pelvis may bleed profusely. Up to 2 liters of blood may be lost from a pelvic fracture. The caregiver should limit motion of the pelvis to prevent further injury. Spinal motion restriction devices are necessary. Procedures such as a log roll may cause significant injury. If a pelvic fracture is suspected (i.e. crepitus, deformity, or pain with palpation) you should consider the use of a scoop stretcher to transfer the victim to the backboard rather than a log roll. This will avoid causing further injury to the blood vessels in that area from compression on the pelvis during the log roll procedure. Injuries to organs within the pelvic cavity can occur with or without pelvic fractures. One should suspect injury with any of the following: · mechanism of injury · pain in pelvic cavity · possible pelvic fracture indicated by instability or crepitus · bloody vaginal or penile discharge Assessment and TreatmentAssessmentHave your patient describe the pain in his own words. It may be described as tearing, dull, sharp, throbbing, or pressure. Ask if the pain started immediately after the injury. Inquire if the pain is getting progressively worse or better. Also ask if what makes the pain worse or better, such as movement, position, or deep inspiration. You will need to remove the patient's clothing to perform your assessment. Inspect for obvious wounds, discoloration, deformity, distention, or pulsation. If a gunshot wound is present, assess for any exit wounds. Gently palpate each abdominal quadrant for tenderness, distention, pulsation, warmth, or coolness. To examine the pelvis, gently press on the iliac crest to assess for pain, instability, or crepitus. TreatmentTreatment of pelvic injuries also require a high index of suspicion as well as supportive care. Treatment for abdominal and pelvic injuries in the pre-hospital environment should include: · Assessment with cervical spine precautions · Administration of high flow oxygen · Treat for shock · Apply spinal motion restriction devices · Rapid and safe transport to the hospital or Trauma Center (Consider EMS helicopter transport) · Initiate ECG monitoring and establish two large bore IV's for vascular access · Consider Medical Anti-Shock Trousers (MAST) for pelvic fractures or for treatment of hypotension - consult your local protocol · Cover any penetrating wounds with moist, sterile dressings and occlusive dressings · Notify medical control and/or receiving hospital. Appropriate and rapid treatment of victims with pelvic and intra-abdominal injuries will decrease morbidity and mortality. Always maintain as a high index of suspicion when victims have suffered as a mechanism of injury that could transmit significant injury to the abdomen or pelvis. Caregivers must remember that these injuries are treated in the hospital setting. Trauma Center EvaluationTrauma center evaluation of these patients may include such procedures as radiographic assessment for the presence of fractures, free air in the abdomen, or blood. The first step in the trauma evaluation will be clearing the cervical spine diagnostically or with an x-ray. Once the C-spine is cleared, a chest x-ray and pelvic x-ray will be performed. Once the pelvis is cleared radiographically, a diagnostic peritoneal lavage (DPL) may be performed. First, a nasogastric (NG) tube must be inserted to evacuate any stomach contents and a Foley catheter will be placed to drain the urinary bladder. The DPL is accomplished by percutaneous insertion of an approximate 6 - 8" catheter into peritoneal cavity and then infusing 1 liter of warm saline via an IV bag and tubing. The bag is then placed on the floor allowing a siphoning return of the liter of saline. The returned saline is then inspected for the presence of blood or white blood cells indicating blood or intestinal perforation respectively. The urinary structures are evaluated by performance of retrograde urethrogram (RUG) if pelvic fracture is present in the male patient. This is usually performed by minimal insertion of a Foley catheter into the meatus followed by insertion of a radiopaque dye. An X-ray is then performed to assess for leakage of the dye into surrounding tissues which could occur secondary to urethral disruption. If the RUG is negative for leakage, then the Foley catheter may be completely inserted. If leakage is detected, then a suprapubic catheter may be inserted by a urologist. A RUG is usually not necessary in female patients as the total distance of their urethra is substantially shorter then that of a male. Computerized Tomography (C/T Scan) evaluation may be utilized as a substitute for some of the above procedures or in conjunction with them. Pre-hospital care should be geared towards rapid assessment and safe transport to the appropriate facility capable of meeting the medical demands of the patient Try our Advanced Abdominal Quiz on the RAEMS Blog (here)
|